


MANY doctors focus on a patient’s individual health at every consultation.
But, in the grand scheme of things, it is really the collective population’s health that is a true measure of our nation’s progress when we speak in terms of achieving millennium goals and sustainable development.

As we continue to increase investment in healthcare, the incidence and prevalence of chronic disease and their complications continue to rise to alarming proportions.
One may say that, the flaw is in the healthcare system itself, which currently results in bare minimum returns in this substantial investment of our budget.
However, if we look at developed countries like the USA and in Europe, the same scenario occurs. Therefore, focusing on healthcare alone and one that is only centered on the individual consultation, means that we are definitely missing the boat where population health is concerned.
Apart from healthcare and its funding, there are other variables that impinge on individual health, which in turn affects population health that may not be obvious to us and, more importantly, our policy makers.
Based on solid research spearheaded by Professor of Epidimology and Public Health at University College London, UK, Sir Michael Mamoth, we have now realised that our health is intimately linked to the social and economic conditions in which we live.
These conditions are shaped by political, social, economic, environmental and cultural forces and can create or destroy our personal health and well-being.
People further down the social ladder usually run at least twice the risk of serious illness and premature death, compared to those at the top.
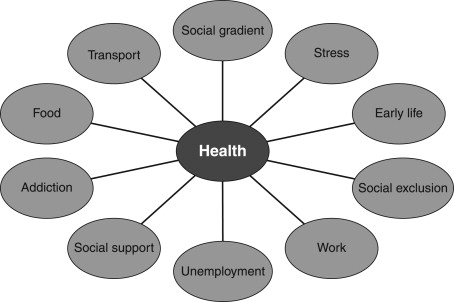
Socioeconomic problems are now viewed as health problems that must be addressed to ensure everyone has the best chance at a healthy life. These conditions are termed the Social Determinants of Health (SDH) and include:
- The Social Gradient (where we find ourselves on the social ladder)
- Unemployment and a lack of job security
- The type of transport available to us
- Early life experience which start before we are born in the form of support received by our parents.
- Social exclusion, poverty, discrimination and prejudice
- The amount of control we have at work
- Addiction to alcohol, drugs and tobacco
- Stress, both at work and everyday life
- The type and quality of food to which we have access
- Our network of social support, at home and in the community’
This means that just investing in healthcare will not solve our health problems, as the SDH show that a vast majority of factors within the non-health sectors affect our health.
Due to our understanding of the SDH we can now see that thinking that our health problems are due to a lack of healthcare is a bit like saying that your broken window is due to the lack of someone to come and repair the window.
We do need healthcare when people get damaged, but it is not lack of healthcare in the first place that leads to people getting ill.
Research into the SDH has revealed that there are inequities in the conditions of daily life that give rise to unavoidable inequalities in health. According to Sir Michael Marmot, “The unequal distribution of health damaging experiences is not any sense a ‘natural’ phenomenon, but is the result of a toxic combination of poor social policies and programmes, unfair economic agreements and bad governance.”
By using the term inequities one gets the sense that it is grossly unfair that we could make a huge difference in health through policy change at an administrative level and we do not. Government policy on health need to focus on these inequities and social justice in its policy, if it is to ever make any noticeable impact on the health of the nation.

We must also remember that our system of governance is also a major factor in determining population health. In a democracy, the ruling party main focus is on reelection.
This means spending today and worrying about debt tomorrow. This results in investment in short-term healthcare plans like; building new hospitals or tertiary care facilities that are tangible to an electorate that is oblivious to the larger submerged part of the iceberg called population health. It is no wonder then, that no matter how many new hospitals we build there will never be enough bed space and patient waiting time continue to become longer.
Clearly, when it comes to population health in T&T, an indicator of Gross Domestic Product, we have been failing in our approach and continue to the same thing expecting a different result. If we are to make any dent in population health, we cannot continue to be guided by negative focusing events and align our political priorities to the SDH.
Reference:
- The Health Gap: The Challenge of an Unequal World: The argument; International Journal of Epidemiology 46(4):1312-1318 · August 2017.
- Social Determinants of Health, the United Nations Commission of Alec Irwin, Jeanette Vega, in International Encyclopedia of Public Health (Second Edition), 2017
Dr Visham Bhimull is a Primary Care Physician MBBS (UWI) Diploma in Family Medicine (UWI)
![]()






